From the research you cite, the test appears useful, but I’m wondering about costs and benefits, as tests not covered by insurance (or at least negotiated rates), tends to be rather expensive.
Consider a 65-year old with no symptoms, a family history including a valve replacement and high cholesterol and a lipid panel such as the attached.
Given these insurance/payment barriers, I think you can get most of the information you need for decision making using the non-HDL-c level from this test, as discussed in the cholesterol article (part 1) on the website.
ApoB can provide a bit more refined risk estimation, particularly in the setting of significant insulin resistance/diabetes and in high-risk treated individuals where there can be significant discordance, but typically isn’t earth shattering for generally healthy individuals compared with non-HDL-c.
I would note that Medicare cites 2010 guidelines while the JAMA article you have cited is 2021. But it’s good to hear that ApoB “typically isn’t earth shattering for generally healthy individuals compared with non-HDL-c”, as a generally healthy individual with a non-HDL-c score under 150. I wouldn’t mind a reasonable cost if it would add meaningful value.
In prior years doctors have mentioned lipo protein A and coronary calcium scores. Do you believe those add much value?
Yes, I looked at the original Medicare link you provided and found that a fair amount of the discussion was a bit dated.
Regarding Lipoprotein(a): we recently did a podcast discussing this topic, episode 191, which may be helpful for you.
Coronary artery calcium scoring is a bit more involved and individualized conversation, although it may be a worthwhile topic for a podcast of its own. I don’t screen broadly using CAC, although it can be helpful to guide treatment decisions (e.g., for lipid-lowering therapies) in patients who are reluctant to take them, or in otherwise “gray areas”.
I’ve read that exercise tends to increase CAC scores, although exercise is clearly helpful in reducing CVD risk. Is that consistent with your view?
The ASCVD risk calculator includes that it is reasonable to initiate statin therapy for all those 55 or older with a CAC score above zero, which seems to make the score not very useful if exercise is likely to result in a non-zero score.
It can, although this tends to be more observed in very-high volume endurance exercisers. I would not expect resistance exercise a few times per week, or low/moderate volume of low/moderate intensity aerobic exercise to have a significant effect on this.
IMO (and in my clinical use), CAC scores tend to be more useful when they conflict with the “expected” finding for a given demographic. For example, a young patient (who should have a CAC of zero, but who actually has a detectable/high CAC score), or an older patient (who would be expected to have some CAC, but who actually has a score of 0). A zero CAC in a young person, or a detectable CAC in an older person (outside of extremes) are less useful for decision making, in general.
My new lipid panel came back a bit better than the one I posted above. My lp(a) test was not so good - 233 nmol/L where standard is < 75. My doctor recommended starting rosuvastatin 10mg and re-checking numbers in three months. Are there any questions I should ask about this med and dosage?
Oops, that should be ** LPAclinicalguidance ** says his raises the risk of a heart attack or stroke by age 80 from 3% to ~7%, assuming I entered numbers correctly.
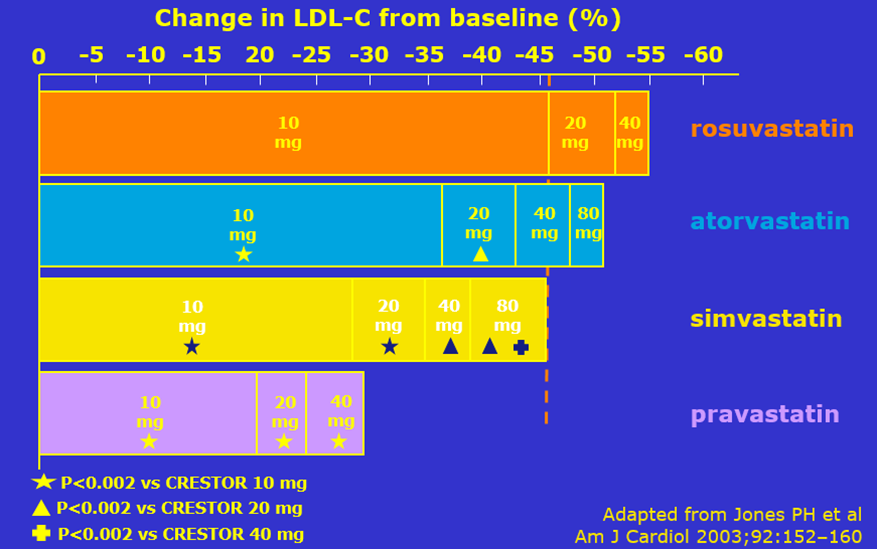
Assuming no significant kidney disease, rosuvastatin 10 mg is typically my preferred starting agent and dose for most folks in a primary prevention situation.
To be clear: this medicine would not be expected to reduce the Lp(a) levels; rather, it is more aggressively controlling the other risk factors given your risk from the elevated Lp(a).
That’s good to hear. Is it the case that, other than possibly PCSK9 inhibitors, there isn’t anything useful to reduce Lp(a) and even that may not actually improve outcomes?
Did you have a chance to listen to our Lp(a) podcast I mentioned above?
The recent SAMSON trial found that upwards of 90% of reported adverse effects of statins are attributable to nocebo-type effects, rather than true drug effects. The overwhelming majority of patients that I treat do just fine with them - as is reflected in adequately blinded, controlled trials.
Additionally, to the extent that true drug side effects occur, they are also dose-related, such that starting on a lower dose (such as 10 mg rosuvastatin) instead of maximum/high-dose therapy (such as 40 mg rosuvastatin or 80 mg atorvastatin) is less likely to cause any issues. It is even possible to go lower with rosuvastatin to 5 or even 2.5 mg, if needed, and to combine this with non-statin therapies (such as ezetimibe, which has essentially no real side effects) to augment the lipid-lowering effect. As a result, 5-10 mg rosuvastatin + 10 mg ezetimibe is a common combination I prescribe to take advantage of the benefits of each at low doses, without risking tolerance issues of maximum dose therapy.
I thought I was reading something else in studies regarding whether meds would improve outcomes. Sorry for the confusion. That podcast is very well done.
The SAMSON study is reassuring. FWIW, I’ve been prescribed 10mg rosuvastatin with the plan to recheck levels in 3 months and alter dosage if appropriate. I’ll discuss your practice of combining two low dose meds rather than one higher dose med with my doctor.
I get very different calculated risk numbers from ** LPAclinicalguidance ** than I do from ASCVD Risk Estimator + (acc.org) on the same inputs. The former gives a risk of a heart attack or stroke by age 80 (14 years) at 3%, while the latter reports a 9% 10-year ASCVD risk. Are they measuring different things?
They are aiming to estimate the same thing - but I’m not sure of the source of your discrepant results. Are you certain you’re putting the exact same inputs into each, with the correct units of measurement? If so, they may be using slightly different models for risk prognostication.
I’m certain I’m inputting the same values (to the extent they ask the same questions). It would seem to be slightly different models, but I’m surprised at the magnitude of the differences.
FWIW, I checked two prescription drug pricing lists and both offered ezetimibe and simvastatin as a combination, while neither offered rosuvastatin in combination. The disparity in ezetimibe cost was astounding (90 days for $16 or $353, similar differences for the combination).
There is a combination product known as Roszet, but I have never prescribed this as the price for the two tablets separately is quite low, and I do not use simvastatin anymore. Consider having your scripts sent to Mark Cuban’s Cost Plus Drugs, where both of these are especially inexpensive. [I have no affiliation with them, but their pricing has been superior for most of my patients]
In the Lp(a) podcast you mention aortic valve stenosis. My father had a valve replaced (in his mid-60s) due to this. At least that worked well for 30 years until it started to regurgitate.
I just thought it odd that simvastatin combination was offered by two sources and neither offered the rosuvastatin combination, but that could be a marketing thing.
Regarding pricing, Ezetimibe (10mg x 90): drug plan, $353; Costco, $18; Cost Plus, $8.40 (+$5 shipping). Rosuvastatin (10mg x 90): drug plan, $3, Costco, $23, Cost Plus, $5.70 (+$5). Costco and my drug plan prices are with shipping (the $16 in my prior post was local pickup).
Thank you again. I likely would never have gotten the Lp(a) test without your information.
This depends on how low I would like to push lipid levels, which itself is related to the individual’s baseline risk. The higher the risk, the more important it is to get levels as low as possible.
For someone with severe elevations in Lp(a), I would probably start the combination therapy to maximize control of the variables I can control.

{kind=link}