Did you have a chance to listen to our Lp(a) podcast I mentioned above?
The recent SAMSON trial found that upwards of 90% of reported adverse effects of statins are attributable to nocebo-type effects, rather than true drug effects. The overwhelming majority of patients that I treat do just fine with them - as is reflected in adequately blinded, controlled trials.
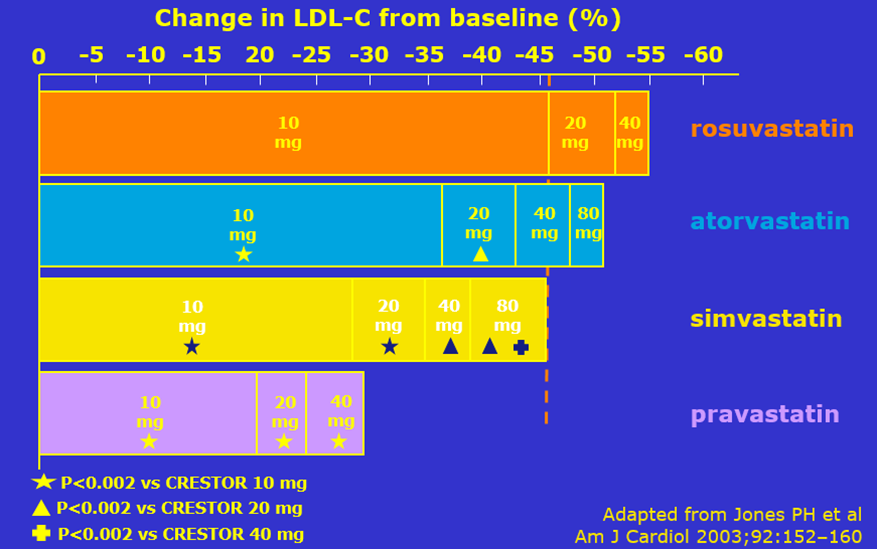
Additionally, to the extent that true drug side effects occur, they are also dose-related, such that starting on a lower dose (such as 10 mg rosuvastatin) instead of maximum/high-dose therapy (such as 40 mg rosuvastatin or 80 mg atorvastatin) is less likely to cause any issues. It is even possible to go lower with rosuvastatin to 5 or even 2.5 mg, if needed, and to combine this with non-statin therapies (such as ezetimibe, which has essentially no real side effects) to augment the lipid-lowering effect. As a result, 5-10 mg rosuvastatin + 10 mg ezetimibe is a common combination I prescribe to take advantage of the benefits of each at low doses, without risking tolerance issues of maximum dose therapy.
{kind=link}