I recently tested very high for Lp(a) - 232 nmol/L with <75 being standard. My lipid panel showed LDL-C at 122 mg/dL and everything else normal. My doctor started me on 10mg rosuvastatin and recommended seeing a cardiologist.
Today I saw the cardiologist, who recommended another lipid panel at 6-8 weeks from when I started statins. If LDL-C is above 70 he recommends increasing rosuvastatin to 20mg. His view is that increasing rosuvastatin has better clinical outcomes than rosuvastatin plus ezetimibe, although the latter produces better test results. How to proceed after an increase would depend on my reaction.
He also said it was not at all clear if PCSK9 inhibitors resulted in better clinical outcomes. He has a patient who was part of a clinical trial following a heart attack and Lp(a) went down during the trials, then went back to the prior level when the trial ended.
Is there anything you’d recommend discussing with the cardiologist under the circumstances?
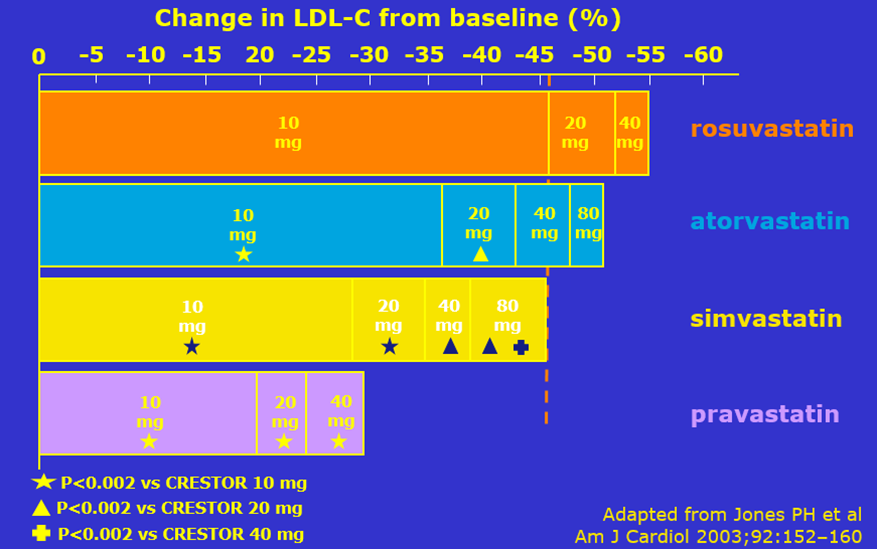
I’m not sure what specific evidence he’d be relying on here. You can see the dose-response effect for statins for yourself, as well as these other references on the topic:
Regardless, there’s still nothing stopping him from adding ezetimibe with or without the 20 mg rosuvastatin, if he wanted to make that increase, in order to get levels to goal.
Not really. The preference on risk calculators is fine; not something I have a strong opinion on here.
While I agree we don’t have direct trials of PCSK9 inhibitors on Lp(a)-mediated outcomes, they are the most effective therapy currently available that do lower Lp(a) levels. I would understand initial reluctance to jump straight to one of these agents, though.
Regarding the last point, it appears that adding ezetimibe is, at worst, not very useful, unless I’m missing something. No real downside, at least some chance of success, would seem to suggest going for it. I would hope this argument, plus the research you cite, would be a convincing approach. Do you have any recommendations for how to deal effectively with a doctor under the circumstances?
I suppose we’ll get another lipid panel, adjust medication if necessary, then figure out how to proceed. At this point I might as well wait for the next lipid panel to raise the points above.
I would not say that adding ezetimibe is “at worst, not very useful”, as it will lower blood LDL-c by about 20%. Correct that there is no real downside as it is generic, cheap, and probably the most well-tolerated of all lipid lowering medicines.
I don’t think I have other advice. If you express your desire to get these levels as low as possible due to concern for Lp(a)-mediated risk, then it is a very reasonable strategy without major downsides. I would not be surprised if they are unaware of this more recent evidence pointing in favor of earlier combination therapy, as these things take time to trickle down to regular practice, even among specialists.
“Combination therapy with statin and a nonstatin LDL-C–lowering agent has been shown to be safe and effective for lowering LDL-C and CV risk reduction in clinical outcome trials.”
“Increasing statin dose is less effective than adding a second agent to lower LDL-C levels; several options are available to personalize therapy (ezetimibe, evolocumab, alirocumab, bempedoic acid, inclisiran).”
My cardiologist suggested I read https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.118.034407, which has a table summarizing various treatments, including high v low doses of a statin, combining different statins and a statin plus ezetimibe. I’m not sure if it’s reasonable to compare results across studies, given differences in design. More aggressive treatments produced better LDL-C levels and ASCVD outcomes, although no statistically significant differences in all-cause mortality.
Yeah, not sure I have much else to add beyond what I’ve already provided, since I’m not really seeing how the reference he provided refutes anything I’ve said.
What gives me pause is looking at the outcomes of the studies citied in ACC 2022 and AHA 2018. The study ACC 2022 cites in support of statin plus ezetimibe, the IMPROVE-IT study, is a study of a population that is different from those who are asymptomatic with concerning blood work. It found a 2 pp (34% to 32%) reduction in serious outcomes, which does not seem all that high. Other non-statin combinations cited in that paper did better, as did other statin therapies (higher doses or two statins) in the studies cited in AHA 2018.
So, on one hand, major organizations recommend ezetimibe plus statin for high risk patients and the marginal LDL-C lowering benefits of higher statin doses are low, on the other hand, looking at outcomes ezetimibe plus statin does not look very impressive, including compared to higher doses or statin combinations.
I hope I don’t sound argumentative. I’m genuinely confused.
There is nothing limiting you from using a higher statin dose. You can do both if you’d like, or pursue other add-on therapy depending on what your cardiologist is comfortable with. In some patients, statin therapy can actually cause a mild increase in Lp(a) levels, although its benefit in that context is moreso mediated by a more substantial reduction in apoB/LDLc levels. And I think the case is fairly clear for which approach tends to produce a more substantial apoB/LDLc reduction.
Additionally, risk reductions are not only proportional to magnitude of blood lipid reduction, but also to the duration that reduction is maintained. This can present an issue when comparing trials, whether they achieved different magnitudes of lipid reduction or if they ran for different durations. The evidence is quite clear that there is consistent reduction in risk per unit of LDL-c reduction, regardless of the method used to achieve it (figure 3, here).
I think your suggestion may be best. Depending on next lipid panel, increase the statin and add ezetimibe. So long as that doesn’t cause side effects problems, it seems the safest and most effective course.
Hello experienced guys, my son is much interested to get herbal certificate from any well-known herbalist school but I’m confused that will it help him in his career? He just cleared 10+2 and looking for some better opportunities but along with that he also wanna take this. What you guys recommend?
{kind=link}